There are a number of options for treating tendinopathy/tendinitis. Initially non-surgical options are explored such as strengthening, eccentric strengthening, ultrasound, deep tissue massage, non steroidal anti-inflammatory medication, dry needling and extracorporeal shock wave therapy. If these do not work, more aggressive and costly treatments such as corticosteroid injections, platelet rich plasma (PRP) injections or surgical paratendon stripping.
Which options have been shown to be effective and cost effective? A meta-analysis of patellar tendon treatment by Chen et al (2019) showed that platelet rich plasma (PRP) injections are more effective than other treatments in terms of functional ability and pain reduction. Dry needling was also shown to be effective for improving functional ability compared to other treatments but not as effective as PRP. The cost of PRP is around £1000 in the UK whereas dry needling costs £50 per session in physiotherapy at current prices at e-physiotherapy. Eccentric loading and other progressive loading exercises for lower limb tendinopathy have been shown to be effective in controlled trials but in meta-analyses, there is variability in the results between studies.
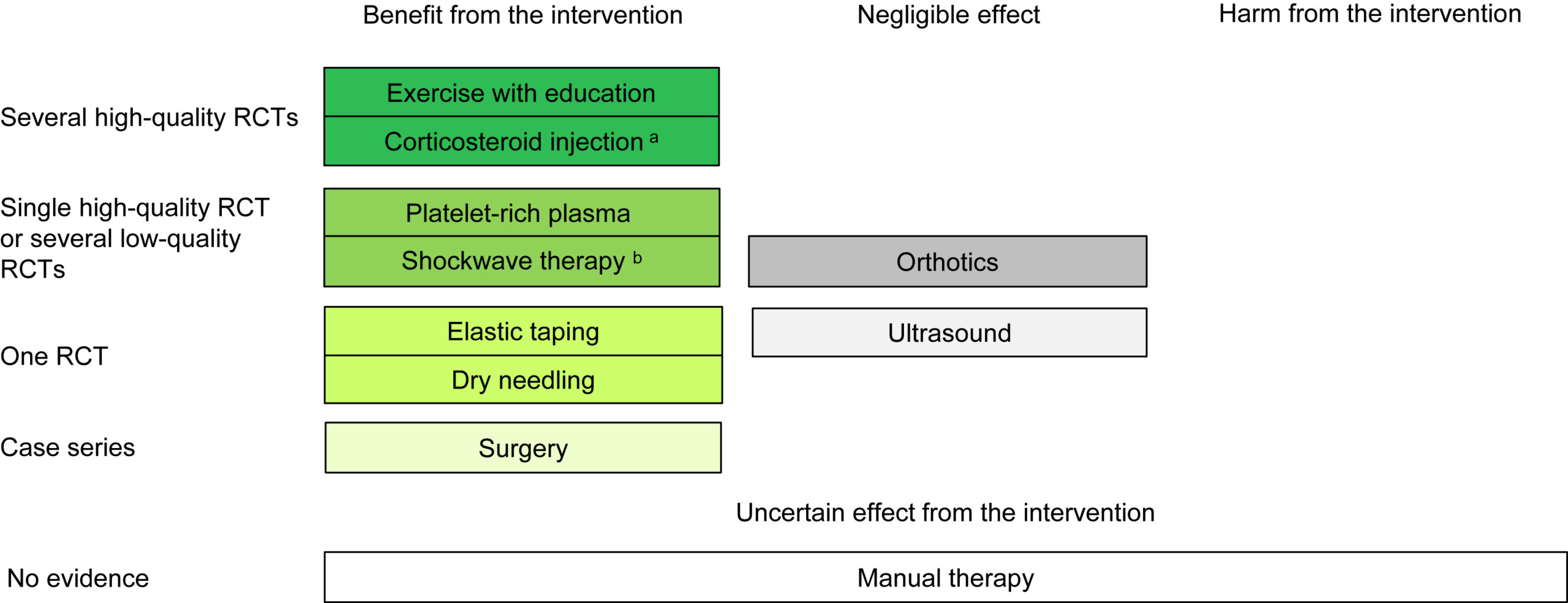
A more recent review of gluteal tendinopathy by Angela M Fearon in the Australian Journl of Physiotherapy, Vol 71, Issue 2, April 2025, pages 81-90, is freely available online and gives a very good review of the current evidence, or lack there of, for management of gluteal tendinopathies. A basic summary of the evidence is the main image for thie article above.
There is good evidence that exercise helps tendinopathy to recover, but which exercises is not clear. An initial reduction in exercise/tendon loading and then a gradual increase in loading can help tendons to recover and this has been know for some time. Treatment needs to be tailored to the individual’s proprioceptive, strength and flexibility deficits, which is difficult to assess in a randomized controlled study. A 2022 study my Mellor et.al. showed that exercise and education with a physiotherapist, had better medium and long term outcomes that a corticosteroid injection or no intervention.
Extracorporeal shock wave therapy (ESWT) has some evidence that it works in tendinopathy, but the quality of some of the studies is poor. It has better outcomes compared to a corticosteroid injection for pain intensity and functional ability. It also has a better outcome when compared to exercise alone. (Ramon et.al 2020).
Dry needling is as effective as a corticosteroid injection for both pain and functional improvment. Brennan et.al. 2017.
Interestingly, tendinopathy for the upper limb is often treated differently to lower limb. Eccentric loading exercises are rarely used and do not seem to be effective. Progressive task specific loading exercises, strengthening adjacent joint muscles, improving coordination are used as the first line of treatment. A systematic review by Challoumas et al (2019) showed that physiotherapy led exercise progressions was effective compared to surgical interventions but that 12 months of treatment may be needed. Surgical intervention for shoulder tendinopathy was no more effective than sham surgery, suggesting that the protocols followed after surgery may be what is effective, not the actual surgery. This includes a period of rest and a progressive increase in loading under physiotherapy supervision.
Definitions:
Platelet rich plasma (PRP) – blood from the patient is centrifuged to separate out and concentrate platelets which are then injected into the tendon to promote healing in the tendon.
Extracorporeal shockwave therapy (ESWT) – sound waves, which are compression waves, are used to mechanically vibrate the tendon and increase blood flow, which in turn helps facilitate tendon healing. The treatment is painful and can be painful for around a week after treatment.
Surgical paratendon stripping – removing the outer covering of the tendon to help reduce nerve fibers growing into the tendon and causing increased pain.
Sham surgery – such as creating incisions for arthroscopy but not actually performing any surgery to the joint or tendons.
Ultrasound (US) – is also sound waves but at a very high frequency that is inaudible to humans. There is no sensation with the treatment unless on a high setting, which may create some heat.
Corticosteroid injection – strong anti-inflammatory medication to reduce tendon inflammation. There is some debate as to how much inflammation is associated with tendinopathy/tendinitis. It was originally thought to be the main factor in tendinitis (hence the name) but it is now thought that there are multiple factors causing tendinopathy, and the name was changed to tendinopathy.
Nonsteroidal anti-inflammatory drugs (NSAIDs) – commonly used examples are ibuprofen, diclofenac and naproxen.
Dry needling – is using acupuncture needles in the tendon to cause small amounts of bleeding and facilitate healing in the tendon.
Eccentric exercise training – is using repeated load on the tendon while it is lengthening. The load is progressively increased on subsequent exercise sessions. How this helps the tendon pain to reduce is not well understood and there are multiple theories trying to explain this, but when researched, these theories do not correlate well with the clinical changes observed, so more research is needed.
References: